


购物车
- 全部删除
 您的购物车当前为空
您的购物车当前为空

 很棒
很棒
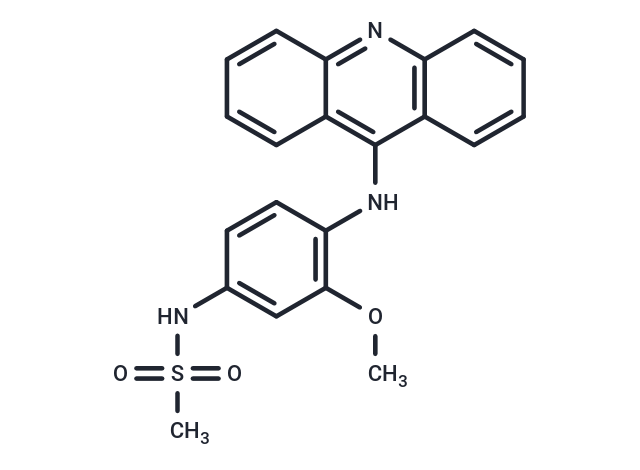
Amsacrine (AMSA) 是一种抗肿瘤剂,可以嵌入到肿瘤细胞的 DNA 中。它还表达拓扑异构酶抑制剂活性,特异性抑制拓扑异构酶 II。
 很棒
很棒Amsacrine (AMSA) 是一种抗肿瘤剂,可以嵌入到肿瘤细胞的 DNA 中。它还表达拓扑异构酶抑制剂活性,特异性抑制拓扑异构酶 II。
| 规格 | 价格 | 库存 | 数量 |
|---|---|---|---|
| 1 mg | ¥ 139 | 现货 | |
| 5 mg | ¥ 297 | 现货 | |
| 10 mg | ¥ 497 | 现货 | |
| 25 mg | ¥ 693 | 现货 | |
| 50 mg | ¥ 897 | 现货 | |
| 1 mL x 10 mM (in DMSO) | ¥ 327 | 现货 |
| 产品描述 | Amsacrine (AMSA) (mAMSA) an antineoplastic agent which can intercalate into the DNA of tumor cells. Amsacrine also expresses topoisomerase inhibitor activity, specifically inhibiting topoisomerase II. |
| 体外活性 | Amsacrine 以浓度依赖的方式抑制HEK 293细胞和非洲爪蟾卵母细胞中的HERG电流,其IC50值分别为209.4 nm和2.0 μM。Amsacrine 使得激活(Δ7.6 mV)和失活(Δ7.6 mV)的电压依赖性发生负向移动。Amsacrine 对HERG电流的阻断不随频率而改变[1]。在体外研究中,不同浓度的m-AMSA作用于正常人淋巴细胞,导致染色体畸变水平从8%增加至100%,SCEs的增加从最低浓度(0.005 μg/mL)时的1.5倍至最高浓度(0.25 μg/mL)的12倍[3]。Amsacrine 诱导的U937细胞凋亡特征为caspase-9和caspase-3的激活、细胞内Ca2+浓度增加、线粒体去极化以及MCL1的下调。Amsacrine 通过减少MCL1的稳定性来诱导其下调。此外,Amsacrine 处理的U937细胞表现出AKT降解和Ca2+介导的ERK失活[4]。 |
| 体内活性 | 在不同剂量的amsacrine(0.5-12 mg/kg)处理的动物中,9 和 12 mg/kg剂量后显著增加了多染性红细胞微核频率。此外,本研究首次证实了amsacrine在体内有高比例的染色体断裂诱导性和低比例的非整倍体诱导性,而nocodazole则表现出高比例的非整倍体诱导性和低比例的染色体断裂诱导性[2]。 |
| 别名 | 安吖啶, m-AMSA, CI-880, AMSA, acridinyl anisidide |
| 分子量 | 393.46 |
| 分子式 | C21H19N3O3S |
| CAS No. | 51264-14-3 |
| Smiles | N(C=1C2=C(N=C3C1C=CC=C3)C=CC=C2)C4=C(OC)C=C(NS(C)(=O)=O)C=C4 |
| 密度 | 1.398 g/cm3 |
| 存储 | Powder: -20°C for 3 years | In solvent: -80°C for 1 year | Shipping with blue ice. | |||||||||||||||||||||||||||||||||||
| 溶解度信息 | DMSO: 50 mg/mL (127.08 mM), Sonication is recommended. | |||||||||||||||||||||||||||||||||||
溶液配制表 | ||||||||||||||||||||||||||||||||||||
DMSO
| ||||||||||||||||||||||||||||||||||||
 比如您的给药剂量是 10 mg/kg ,每只动物体重 20 g ,给药体积 100 μL , 一共给药动物 10 只 ,您使用的配方为 5%
比如您的给药剂量是 10 mg/kg ,每只动物体重 20 g ,给药体积 100 μL , 一共给药动物 10 只 ,您使用的配方为 5%  DMSO+ 30%PEG300+ 5%Tween 80 + 60%Saline/PBS/ddH2O, 那么您的工作液浓度为 2 mg/mL 。 母液,添加 300 μLPEG300 混匀澄清,再加 50μLTween 80, 混匀澄清,再加 600μLSaline/PBS/ddH2O 混匀澄清
DMSO+ 30%PEG300+ 5%Tween 80 + 60%Saline/PBS/ddH2O, 那么您的工作液浓度为 2 mg/mL 。 母液,添加 300 μLPEG300 混匀澄清,再加 50μLTween 80, 混匀澄清,再加 600μLSaline/PBS/ddH2O 混匀澄清 以上为“体内实验配液计算器”的使用方法举例,并不是具体某个化合物的推荐配制方式,请根据您的实验动物和给药方式选择适当的溶解方案。
 嗨!有任何问题?点我咨询
嗨!有任何问题?点我咨询
评论内容